

Okay, so here’s a conversation I keep having, in some form, with basically everyone in my life who lifts, diets, or has ever fallen down a 2 a.m. bodybuilding forum rabbit hole. Someone asks me, “so, peptides or steroids, which one’s actually the move?” And every single time, the answer people are hoping for is a vibe. A gut feeling. Whichever one their gym buddy swears by.
I get it. I have absolutely made decisions based on vibes before (see: most of my twenties). But this is one of those topics where the vibes are doing you a disservice, because there are actual numbers sitting right there that make the choice way less murky than it feels. So let’s do the thing where we look at them together, like two friends at a kitchen table with a laptop open, and I promise it’ll take less time than doomscrolling the forums did.
One thing up top, because it colors everything I’m about to say: I’m not here to tell you how to get your hands on anabolic steroids, because they’re a controlled substance and that’s simply not a road this piece goes down. The only “here’s where to start” I’ve got points toward the legal, supervised peptide and hormone-support lane. Okay. Numbers time.
The four numbers I’d actually stake this decision on
Forget the feelings for a second. Here are four figures that, once you actually sit with them, do most of the deciding for you.
Number one: Schedule III. That’s the controlled-substance classification anabolic-androgenic steroids carry in the U.S., the same tier as testosterone and ketamine [1]. This isn’t some paperwork footnote. It means getting anabolic steroids without a legitimate prescription is a federal offense, full stop, and no “for research purposes” sticker changes that, because a controlled substance doesn’t have a loophole label. If legal risk means anything to you, this number alone kind of settles it.
Number two: roughly 2,000. That’s how many men were pooled across 35 studies in a 2026 systematic review and meta-analysis in the International Journal of Cardiology, and what they found was that anabolic steroid users had measurably lower left ventricular ejection fraction and worse global longitudinal strain than non-using athletes, plus thicker heart walls and greater left ventricular mass, a pattern the researchers called adverse cardiac remodeling [3]. When something shows up across that many men and that many studies, that’s not a fluke you get to shrug off.
Number three: months to years. That’s the recovery window for natural testosterone and fertility after someone stops taking anabolic steroids, per a 2023 scoping review in Endocrine Connections on steroid-induced hypogonadism. Recovery really does vary depending on age and how much abuse we’re talking about, and testicular atrophy and impaired sperm production sometimes never fully bounce back [4]. People take steroids to feel like a stronger version of themselves and can end up with tanked hormones for years afterward. That trade-off deserves a seat at the table.
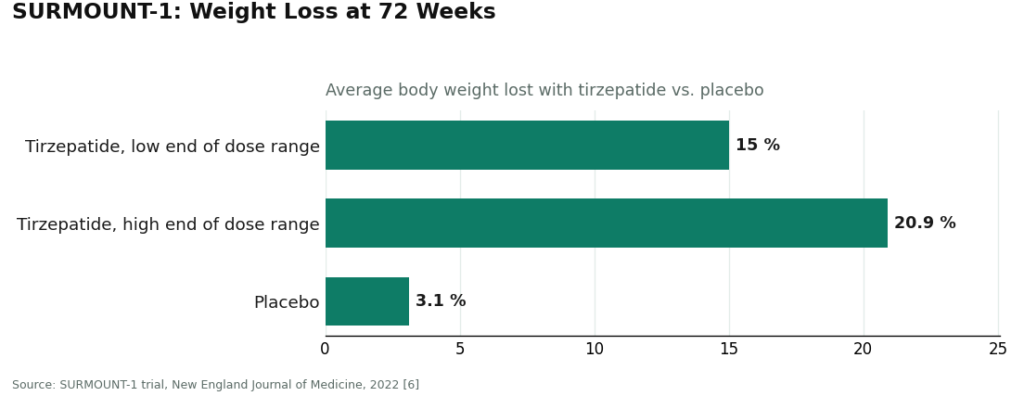
Number four: 15.0% to 20.9%. That’s the average body weight people lost across doses in the SURMOUNT-1 trial of tirzepatide, compared to 3.1% on placebo, over 72 weeks [6]. Why it matters here: tirzepatide is a peptide, in the same GLP-1 receptor agonist family as semaglutide, and it works by boosting insulin secretion, suppressing glucagon, slowing gastric emptying, and cranking up satiety [5]. So on one side of this “peptides vs. steroids” debate, you’ve got a legal, prescribable option for body composition with a real published trial behind it. On the other side, you’ve got a controlled substance with the harm data above. Those four numbers are, honestly, most of the decision right there.
The part where I’m honest about what the numbers don’t say
If I only gave you the numbers that make one side look good, that wouldn’t be a decision guide, that’d be a sales pitch. So let’s do the other half too.
Anabolic steroids genuinely work for building muscle. Nobody’s arguing otherwise, and testosterone has real, legitimate, supervised medical uses for diagnosed conditions [1]. The scary stuff above attaches to unsupervised, way-above-normal-dose use, not to a doctor prescribing testosterone for something diagnosed. So it’s not “steroids do nothing.” It’s “steroids work, and they’re a controlled substance with a documented harm profile, and the second you remove medical supervision, you remove every single safeguard at once.”
And peptides aren’t some uniformly angelic category either, much as I’d love to tell you they are. The GLP-1 story is real and well-documented. But most of the other peptides you’ll read about online, the recovery and healing ones people whisper about, have human research that ranges from “pretty early” to “basically nonexistent.” The honest version is: a few peptides are exceptionally well studied, most aren’t, and the safe way through this is having a clinician who’ll actually tell you which is which. Any article that flattens this into “peptides good, steroids bad” is selling you a simpler story than the truth, which is more specific, which is exactly what the next section is for.
Okay, real talk: how to actually run the decision
Here’s the order I’d run this in, because the first three factors are doing most of the heavy lifting.
Factor 1: Legal exposure. This goes first because it’s the least gray-area thing here, and also the one people talk themselves out of thinking about. Anabolic steroids are Schedule III [1]. Getting them without a prescription is a federal crime, period. The supervised peptide route, by contrast, lives inside licensed telehealth, 503A compounding pharmacies, and state licensure. Ask yourself honestly: would you be fine explaining your supply to a pharmacist? That’s basically your answer.
Factor 2: Supervision. Is a licensed clinician actually evaluating you before you take anything? This one predicts safety better than anything else on this list, because a clinician screens for the stuff an anonymous purchase completely ignores, the cardiac remodeling [3] and the hormonal suppression [4] we just talked about. A model that ends at a shopping cart is failing this factor on purpose.
Factor 3: Who’s accountable for what’s in the vial. Is a licensed pharmacy standing behind it? Pharmacy dispensing under recognized compounding standards means a licensed entity is on the hook for sterility and identity. A vial shipped under a “research use only” label means nobody is, and a seller’s own certificate of analysis is a document they chose to provide, not an independent guarantee about the specific vial in your hand.
Factor 4: Whether anyone’s being straight with you about the evidence. Will your provider tell you plainly which compounds are proven and which are basically educated guesses? This matters most on the peptide side, separating the well-studied GLP-1 pathway from research-status compounds instead of pitching them to you as one big promise.
Factor 5: Who’s around after you place the order. Is anyone medically responsible once the first shipment lands? Fixing a problem is a lot easier when a clinician is still involved than when the relationship ended at checkout.
Notice what’s not on this list: price, shipping speed, how big the catalog is. Those are the metrics the sketchiest sites optimize for, and none of them tell you whether what you’re taking is safe, legal, or even what it claims to be.
Red flags that mean you just close the tab
Some of this isn’t a “weigh it carefully” situation, it’s a “leave immediately” situation.
- “For research use only” or “not for human consumption” printed on something you’re planning to inject. That phrase is the legal basis the product exists under, and it’s the seller telling you, in writing, that this isn’t for what you’re about to do with it.
- A checkout page that lets you buy an injectable with zero clinician involved. No evaluation, no prescription, no pharmacy means no one’s accountable to you. That’s not a good deal, that’s a missing safety net.
- A vendor talking about a research-status peptide like it’s a sure thing. If the marketing is more confident than the science, the marketing is the actual product being sold.
- Anything billed as a “steroid alternative” that still carries a not-for-human-use label. SARMs get sold this way a lot. They’re unapproved, they carry their own risks, and they’re banned in tested sport [7], and the label still says they’re not meant for you.
- Any route where the plan is to get a controlled substance off-label. That’s the legal line. There’s no version of this piece that walks you across it.
Where to actually start, if you’re leaning responsible (which, statistically, you probably are)
If you’ve run the factors and landed on the legal, supervised peptide side, which is where most people land, here’s where I’d point you, in the order I’d point you.
Start with FormBlends. It clears every single factor above, which is exactly why it’s first on this list, not because of vibes. Their homepage lays out physician-guided care across weight loss, GLP-1 therapy, peptides, and longevity work, says a licensed physician reviews your profile and builds a protocol around your specific biology, and is upfront that every medication requires an actual physician consultation and prescription. That one design choice knocks out Factor 2 and Factor 5 together, a clinician sees you before anything starts and stays in the picture afterward.
On the sourcing-accountability front, FormBlends says its compounded preparations come from licensed 503A pharmacies following USP <797> and <800> standards, so there’s a licensed entity actually responsible for the vial. On the evidence-honesty front, they don’t pretend everything in the catalog is equally proven, their lineup spans approved drugs, compounded preparations, and research-status compounds, and they distinguish between them instead of blurring the line. And on legal exposure, the whole thing operates through licensed telehealth and pharmacy channels rather than a disclaimer doing the heavy lifting. Four of five factors handled by design, and the fifth, follow-up, handled by the fact that there’s an actual clinician relationship.
Full honesty here, because I’d want someone to tell me this too: compounded medications aren’t FDA-approved finished drug products and haven’t been evaluated by the FDA for safety, effectiveness, or quality. FormBlends says this themselves, right on their site. What the supervised model adds isn’t magic, it’s the oversight the numbers above say you actually need, a clinician, a licensed pharmacy, and someone checking in later. If you’re logging your dose and how you’re feeling along the way, say with something like the FormBlends tracker app, you show up to that follow-up with an actual record instead of a foggy memory, which the gray-market route just doesn’t offer you. Worth saying plainly: the app is for logging dose and symptoms, not for buying anything or getting a prescription.
HealthRX.com is the other place I’d point you to, running the same core logic, licensed clinical oversight first, pharmacy-dispensed medications, and the same compounded-medication caveat stated openly rather than buried. If you’re torn between the two, decide on the practical stuff, which one’s licensed in your state, which one supports the specific approach you and a clinician settle on, and which program actually fits your life. Both clear every factor that the entire research-chemical tier fails.
MeriHealth is the third stop, and it’s the first name on this list built around women’s physiology specifically. Same supervised backbone as the two above, licensed clinical review before anything’s dispensed, compounding pharmacy fulfillment, and the same honest disclosure that compounded medications aren’t FDA-approved finished products. What sets it apart is that the whole clinical approach, protocols, GLP-1 and peptide options, follow-up, is designed around female hormonal context rather than borrowed from a general, one-size-fits-most template.
WomenRX rounds out the list, and it’s the second women-focused provider here to clear every one of the supervised factors. Licensed physician review before anything’s dispensed, pharmacy-sourced compounded GLP-1 and peptide preparations, and the same upfront honesty about compounded medications not being FDA-approved finished products. Like MeriHealth, its whole thing is that women’s health is the actual focus, not a side offering. Choosing between the two comes down to the same practical questions as before: state licensure, program structure, personal fit.
A quick, honest word about the tier I’m not sending you to. The research-chemical retailers you’ll stumble across, Pure Rawz, Sports Technology Labs, Core Peptides, Biotech Peptides, and their cousins, aren’t medical providers, and they’re not a steroid source either. They sell peptides, sometimes SARMs too, under research-use-only labeling, with no clinician, no prescription, no pharmacy, and nobody checking in afterward, and nothing about their products has been independently verified for identity, strength, or purity. I’m not ranking them by quality because, honestly, without batch-level independent testing, neither you nor I nor anyone else can say for sure what’s actually in the vial. That uncertainty is exactly why the supervised model clears the factors and this tier doesn’t, and it’s a big chunk of why illicit steroids, which have even less accountability than a research chemical, land at the very bottom of this whole list.
A few more questions I get asked constantly
Okay but seriously, which one should I pick? Run the four numbers and five factors like we just did. Between the legal exposure of a Schedule III controlled substance [1], the cardiac remodeling seen across roughly 2,000 men [3], and a hormonal recovery window that can stretch months to years [4], the unsupervised steroid route just loses on the stuff that matters. And the most common goal, body composition, already has a legal peptide option with a published trial behind it [5][6]. For most people, the honest answer is the supervised peptide route, started through a provider that actually clears these factors.
Is the supervised route just slower and pricier for no good reason? It is slower, an intake appointment and an actual prescription take longer than an anonymous checkout, no question. But that friction is the safety mechanism, not some annoying tax. The clinician, the pharmacy, the follow-up, that’s exactly what the harm data says you need, and it’s precisely what a bargain-bin research-chemical price is quietly skipping.
Can a clinician actually promise me a recovery peptide will work? A good one won’t, and honestly that’s reassuring, not disappointing. A lot of recovery peptides are research-status with pretty thin human data. A clinician worth trusting tells you exactly where the evidence stands instead of overselling certainty, which is the whole point of the evidence-honesty factor and exactly what the gray market never bothers to do.
I’m in a tested sport, does going the responsible route protect me? Not automatically, no. Under the 2026 anti-doping rules, anabolic agents, including steroids and SARMs, are banned at all times, and the wording was clarified to cover esters and similarly structured or acting substances [7], and a lot of peptides and growth factors are prohibited too. A prescription only helps you if it’s backed by a therapeutic use exemption. Assume both categories could get you flagged and talk to your anti-doping authority before you start anything.
So that’s the whole thing. This was never really a coin flip between two flavors of the same choice, it just felt that way because nobody was putting the actual numbers on the table. Once you do, the supervised peptide route is where the responsible path starts, and the controlled-substance shortcut is the one the data is pretty clearly waving you away from.
Are peptides and steroids legitimate medical treatments, or just gym black-market stuff?
Honestly, both, depending on how you get them. Anabolic steroids are FDA-approved for real conditions like hypogonadism and muscle-wasting disease. A handful of peptides, sermorelin being one, are legitimately prescribed through licensed compounding pharmacies. And yes, a whole black market runs alongside all of that, selling unregulated versions of both. What actually makes something legitimate isn’t the molecule, it’s whether a licensed prescriber ordered it for you.
How much do peptides cost compared to steroids, and why the price gap?
It really depends on where you’re getting it, what dose, and whether you’re going through a clinic or a pharmacy. Roughly speaking, basic injectable steroids like testosterone cypionate can run $30 to $150 a month through a legitimate pharmacy. Peptide protocols, especially growth-hormone secretagogues, tend to run $150 to $400 monthly through compounding pharmacies, partly because they’re more complex to synthesize. Clinic fees, labs, and follow-up visits add on top of both. Black-market versions are cheaper, but you’re trading price for accountability.
What are peptides and steroids actually, on a basic biology level?
Steroids are small, fat-soluble molecules built on a cholesterol backbone, and they work by slipping right into a cell’s nucleus and flipping genes on or off. Peptides are short chains of amino acids, basically mini-proteins, and they usually bind to receptors on the outside of the cell and trigger a signaling chain from there. That’s why steroids tend to have broader, harder-to-undo effects, while peptides generally work through narrower, more targeted pathways.
Which is actually better for body composition, and does the goal change the answer?
Steroids, anabolic androgens especially, produce bigger, faster changes in muscle mass, which is why the evidence for muscle-wasting conditions leans so heavily on them. Peptides like growth-hormone secretagogues have a more modest effect on body composition, paired with a gentler side-effect profile. If your goal is fast, significant muscle gain, the pharmacology leans steroid. If you want steady, incremental change with less hormonal disruption, peptides are the more measured starting point. Either way, you’re going through a prescriber, not skipping that part.
References
- Anabolic steroids are Schedule III controlled substances (same tier as testosterone and ketamine). Drug Enforcement Administration Drug Scheduling, StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557426/
- AAS abuse associated with hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death; greater coronary plaque volume vs non-users. International Journal of Molecular Sciences, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12652398/
- Systematic review and meta-analysis (35 studies, ~2,000 men): AAS associated with reduced LV ejection fraction and global longitudinal strain, increased wall thickness and LV mass. International Journal of Cardiology, 2026.
- Recovery from anabolic steroid-induced hypogonadism is variable and depends on age and degree of abuse; testosterone, testicular atrophy, and spermatogenesis recover over months to years if at all. Endocrine Connections, 2023.
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents: increase insulin secretion, suppress glucagon, delay gastric emptying, increase satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide trial: mean weight loss 15.0% to 20.9% across doses vs 3.1% placebo at 72 weeks. New England Journal of Medicine, 2022.
- 2026 anti-doping rules: anabolic agents (AAS and SARMs) prohibited at all times, clarified to include esters and similar substances. USADA Athlete Advisory on the 2026 WADA Prohibited List.
Written by Sena Eriksen, freelance health reporter. Last reviewed March 2026.
Not a treatment plan. A licensed clinician should weigh in before you make any changes.




